Subarachnoid haemorrhage
Causes
Investigations
Complications
Management
*the way nimodipine works in subarachnoid haemorrhage is not fully understood. It has been previously postulated that it reduces cerebral vasospasm (hence maintaining cerebral perfusion) but this has not been demonstrated in studies
- 85% are due to rupture of berry aneurysms (conditions associated with berry aneurysms include adult polycystic kidney disease, Ehlers-Danlos syndrome and coarctation of the aorta)
- AV malformations
- trauma
- tumours
Investigations
- CT: negative in 5%
- lumbar puncture: done after 12 hrs (allowing time for xanthochromia to develop)
Complications
- rebleeding (in 30%)
- obstructive hydrocephalus (due to blood in ventricles)
- vasospasm leading to cerebral ischaemia
Management
- neurosurgical opinion: no clear evidence over early surgical intervention against delayed intervention
- post-operative nimodipine (e.g. 60mg / 4 hrly, if BP allows) has been shown to reduce the severity of neurological deficits but doesn't reduce rebleeding*
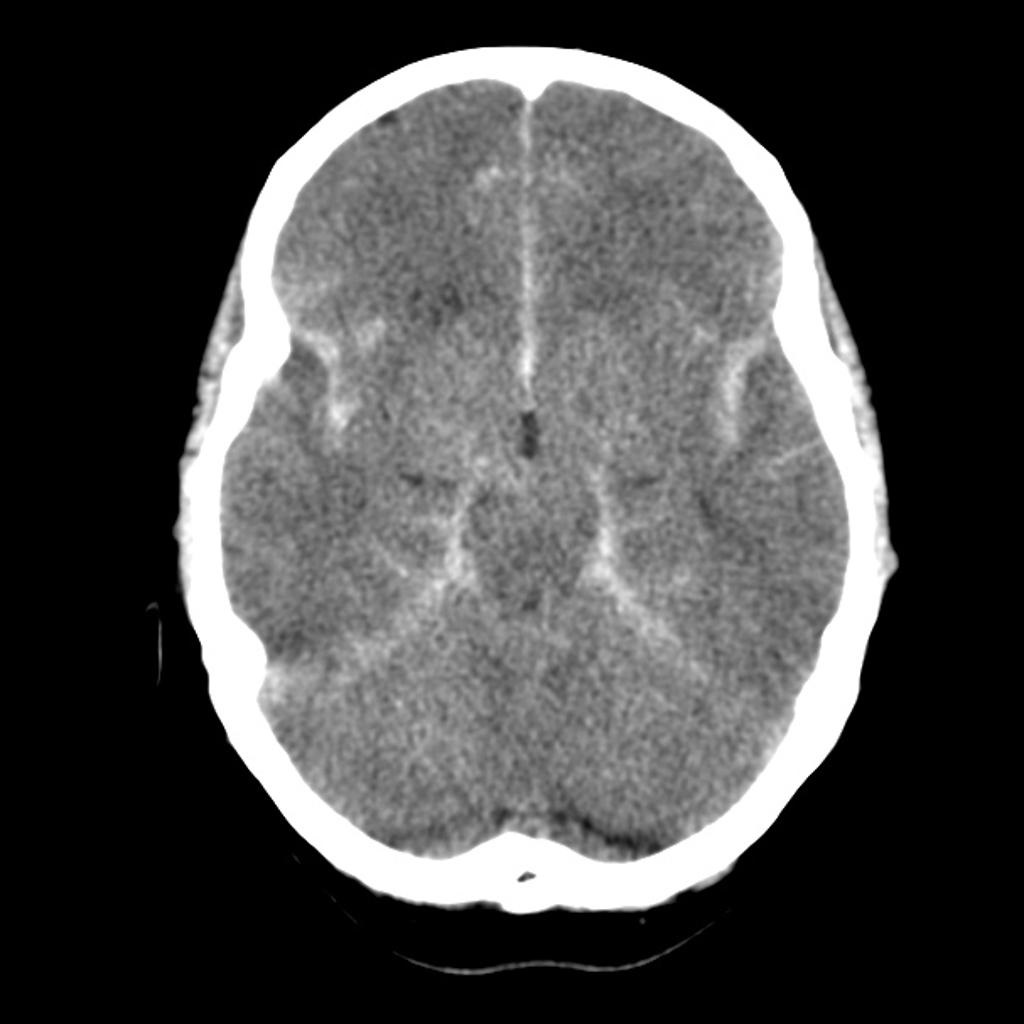 | |
| © Image used on license from Radiopaedia | |
CT image shows diffuse subarachnoid haemorrhage in all basal cisterns, bilateral sylvian fissures and the inter-hemispheric fissure. This case demonstrates the typical distribution that takes the blood into the subarachnoid space in a subarachnoid hemorrhage.
*the way nimodipine works in subarachnoid haemorrhage is not fully understood. It has been previously postulated that it reduces cerebral vasospasm (hence maintaining cerebral perfusion) but this has not been demonstrated in studies

